
We stumble upon them, unpredictably, in certain life situations or during a side course of professional research. The blank spots on the map of needs represented by the built environment.
Rehab care sector is one of them. It is often dealing with social stigma, to such extents, that even deliberate research leaves one with an impression, that there is very little straight-forward talk on the subject.
This work’s overall intention is to look for solutions which will provide suitable rehab care, to those previously underserved.
The hope that an example of thoughtful and inclusive design for a rehab facility can contribute to changing the current state of things and provide a more supportive built environment for the troubled members of the society, became the point of departure for this research.
research question
How to make rehab care more accessible in rural areas and for the underserved groups of patients with the development of dedicated infrastructure?
background
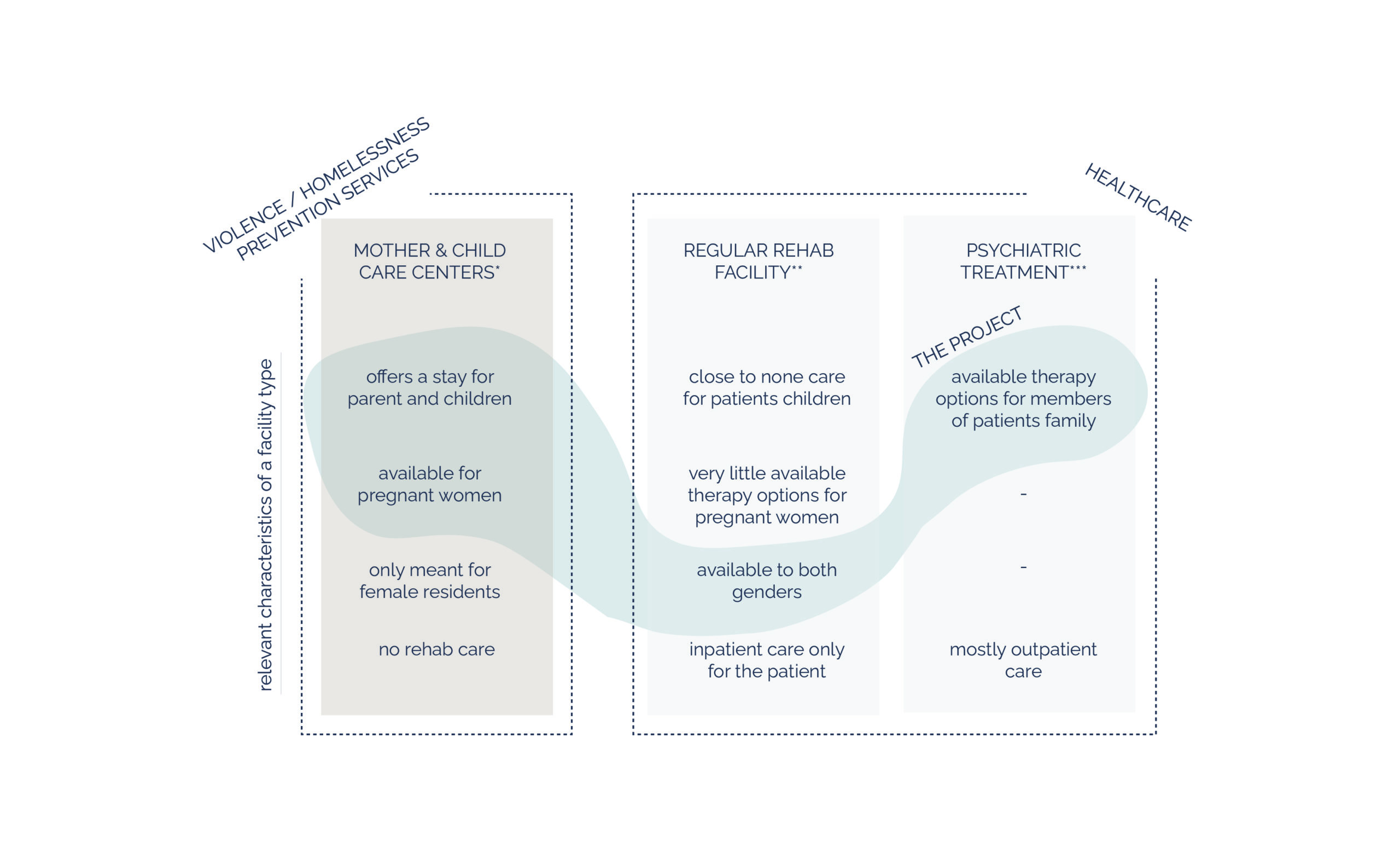
In the course of research, I found that rehab patients who suffer from co-occuring mental disorders, often are not able to receive suitable treatment for both conditions, at the rehab-oriented facilities.
At this time, the first cross-sector bridge was drawn in my mind. In terms of the function that I wanted my building to serve, it appeared crucial to join parts of rehab care and psychiatric treatment facilities operations, binding together two sectors of healthcare.
The other problem which became apparent to me, when gathering the information for the project, was the lack of rehab tailored to the needs of pregnant women and as an extension of that topic – parents, caring for underaged children, who do not have a possibility to admit into inpatient facility, due to lack of childcare options.
Furthermore, the children themselves often require specialised help, coming from co-addiction syndrome, which could be addressed during their ( and the parent’s ) stay at the facility.
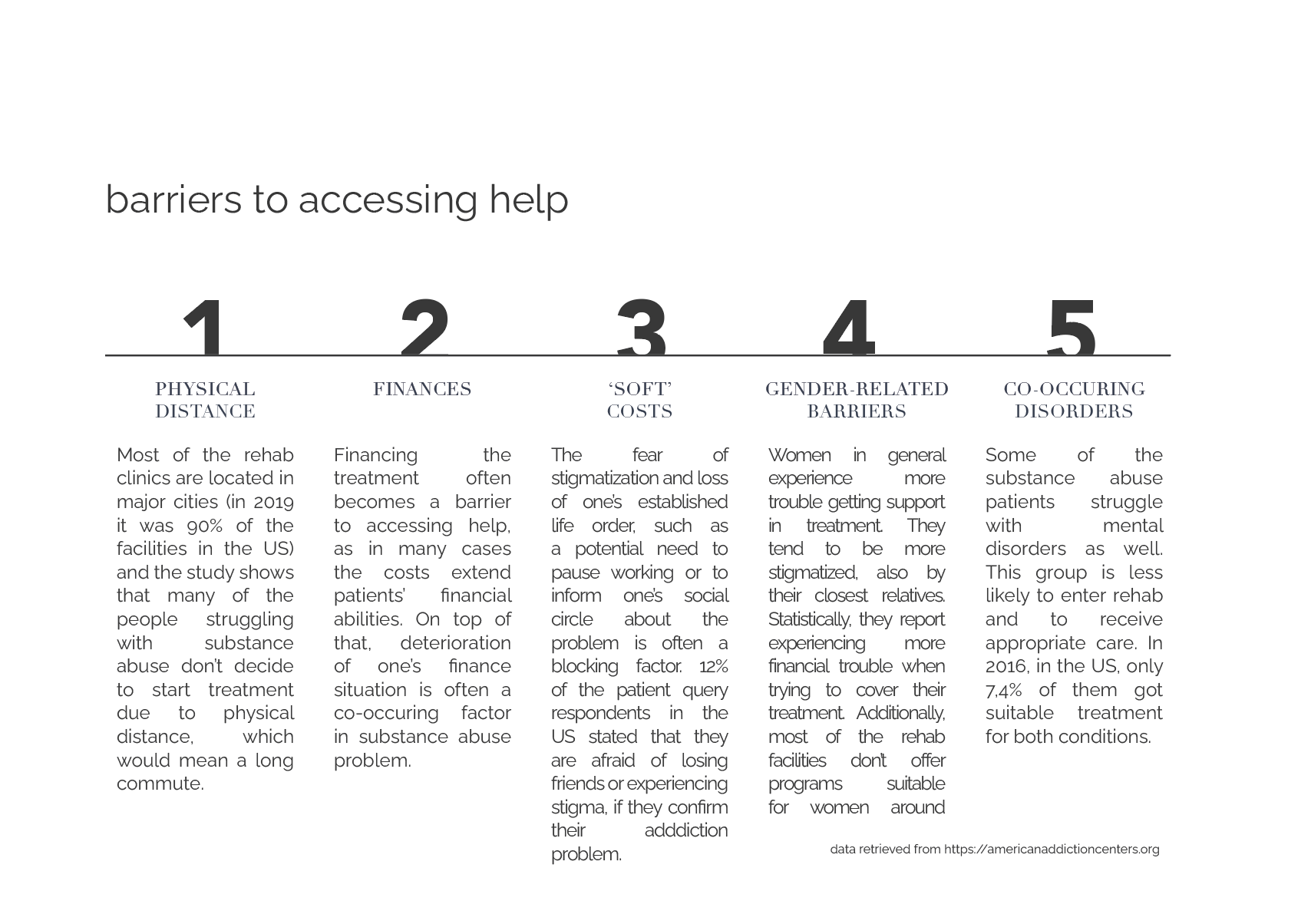
As the next step, I have gathered together the main barriers to accessing help.
The patients often report difficulties tied to the need to commute to a city, the financial aspect and the fear of losing their appearances, if they officially admit into treatment.
As mentioned before, there is also lack of suitable care programmes for women who are mothers to small children and an absolute lack of such for the pregnant ones.
Moreover, most facilities don’t offer suitable care to patients with double diagnosis, which means the co-occuring mental disorders.
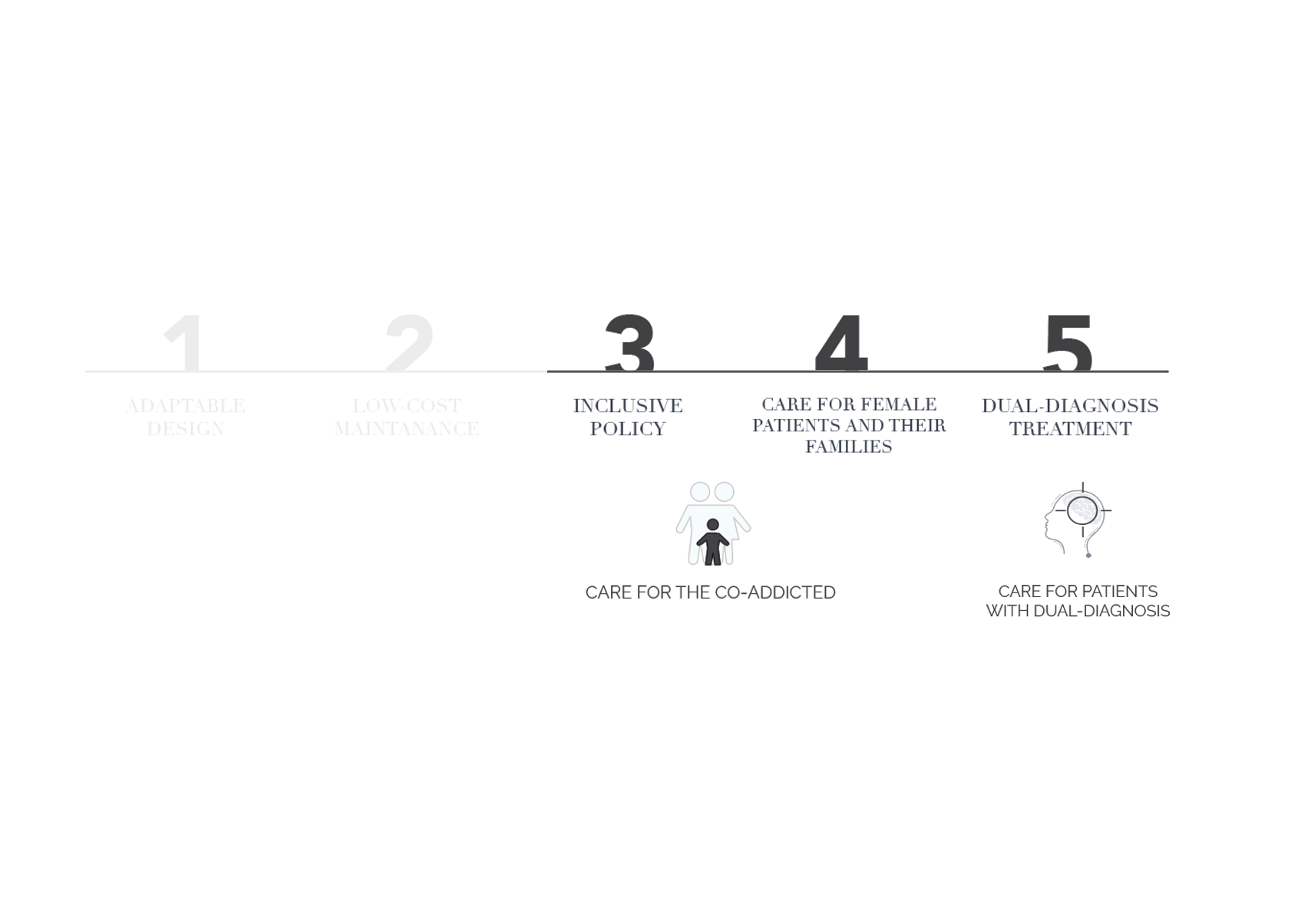
At this point, I was able to identify the project’s target group, being the rural communities and, among and beyond those, the patients with dual-diagnosis, women around pregnancy, underaged children of the patients and multiple cases of co-dependance.
As one of these categories refers to a spatial factor ( the need of more care accessibility in the rural areas) and the others respond to the need of a tailored patient care, I decided to subdivide the concept, along with the project goals and strategies, into two parts: the patient care and the architectural side.
concept – patient care
Those strategies are an answer to the previously identified barriers to accessing help.
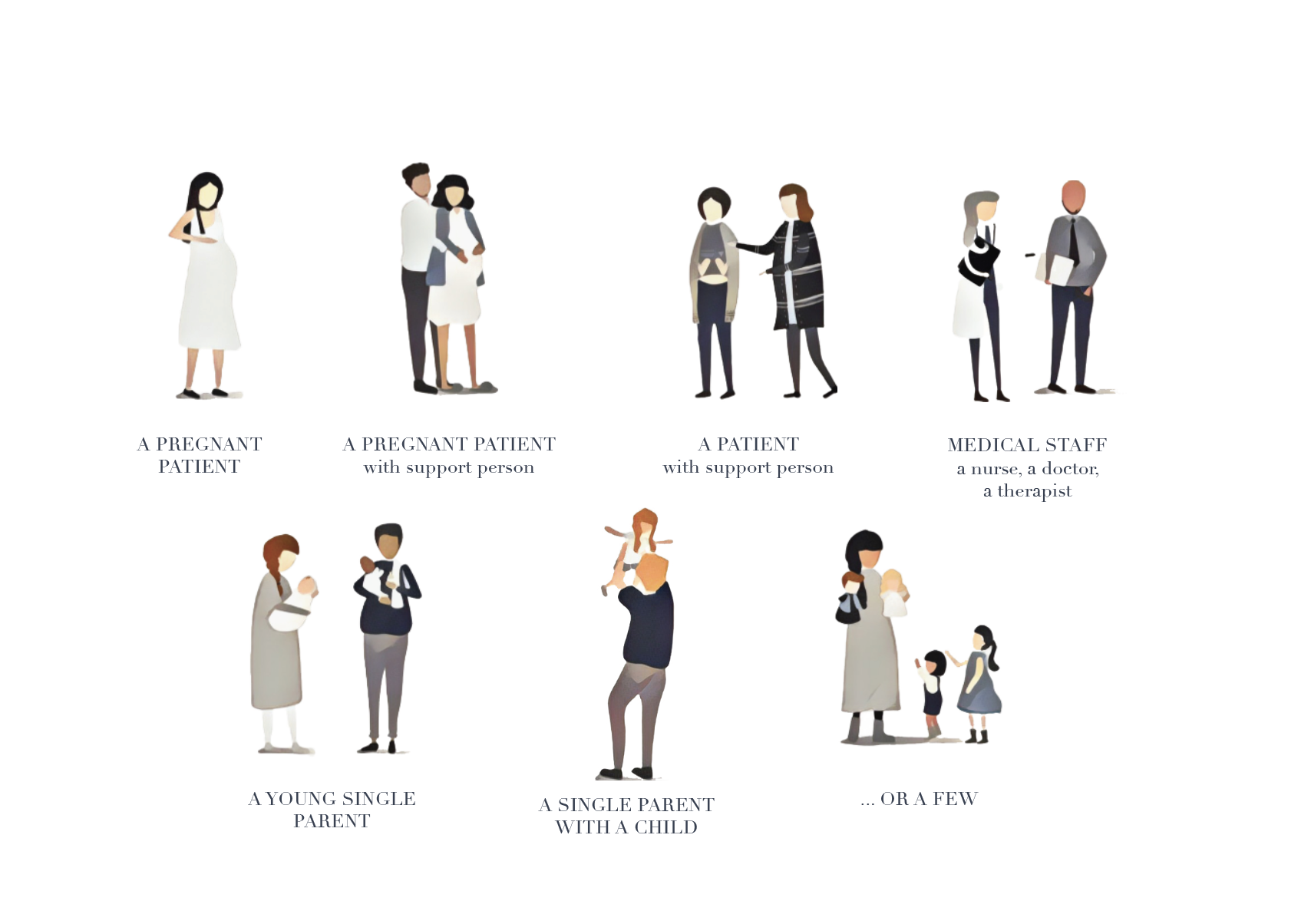
The factor distinguishing my facility concept from a regular rehab is the capacity to host groups of patients, including children. I identified some possible groups, coming in and I tried to assign the specific needs to them, which helped me in creating the functional programme for the building.
patient groups
concept – architectural
Now, we arrive at the architectural side of the concept. The focus laid with providing the locally available care and therefore, coming up with a modular, replicable facility, which could be adapted to many sites.
Therefore my strategies were to design a facility versatile in form and expression, which could also offer a low cost version, for rural communities, who don’t work with big budgets.
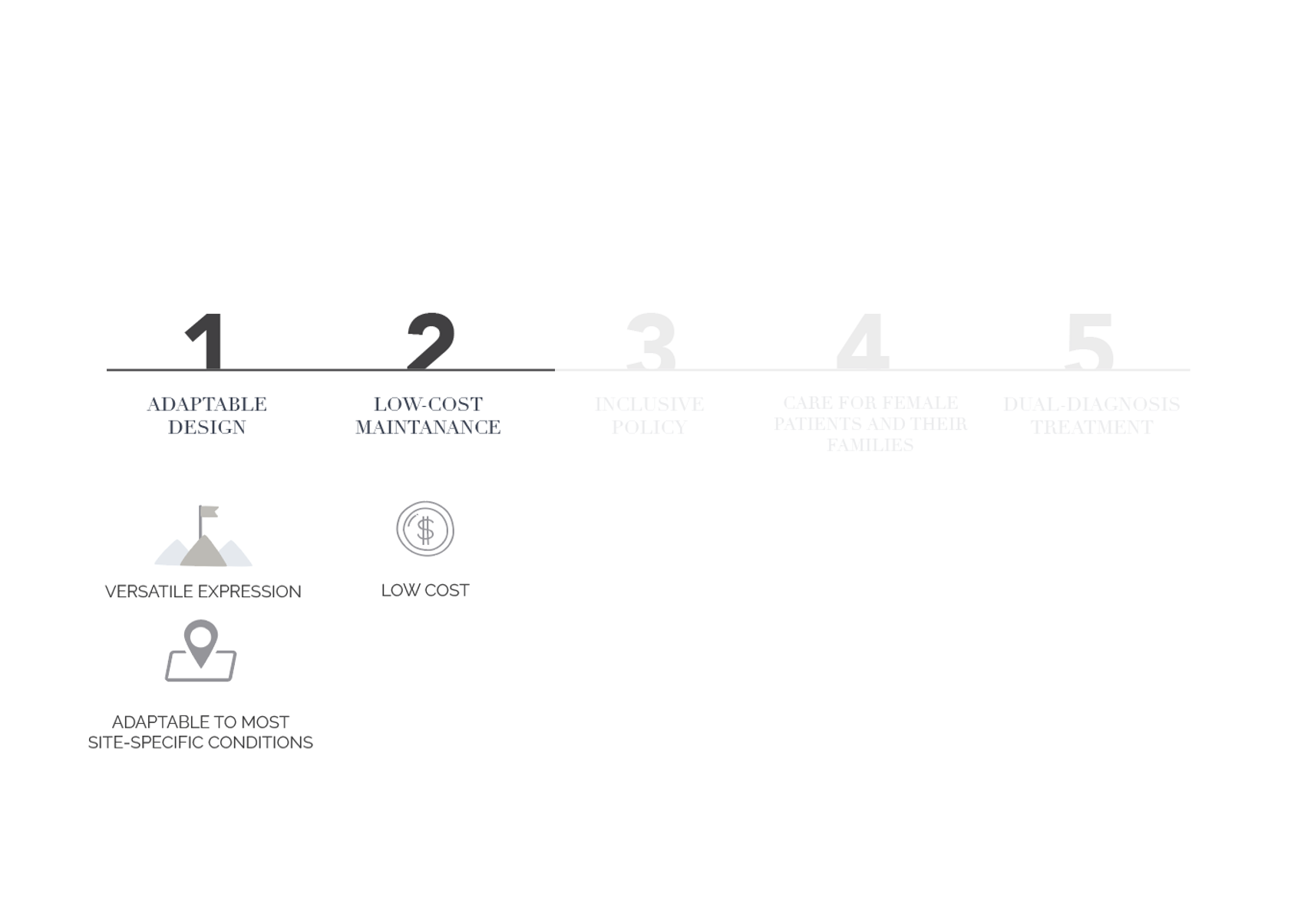
This led to an idea of expandable design, which would allow for three versions, going from most modest and affordable one, to an extra comfortably equipped one.
COMPACT – REGULAR – EXTENDED
This size division is visible in three aspects of the design, being the availability of functions, the architectural features, and the recommendations for picking a site.
The project led to what’s essentially a design for three different buildings, the guidelines for placing each of them on a suitable site and the pattern of expansion between the consequent options.
design
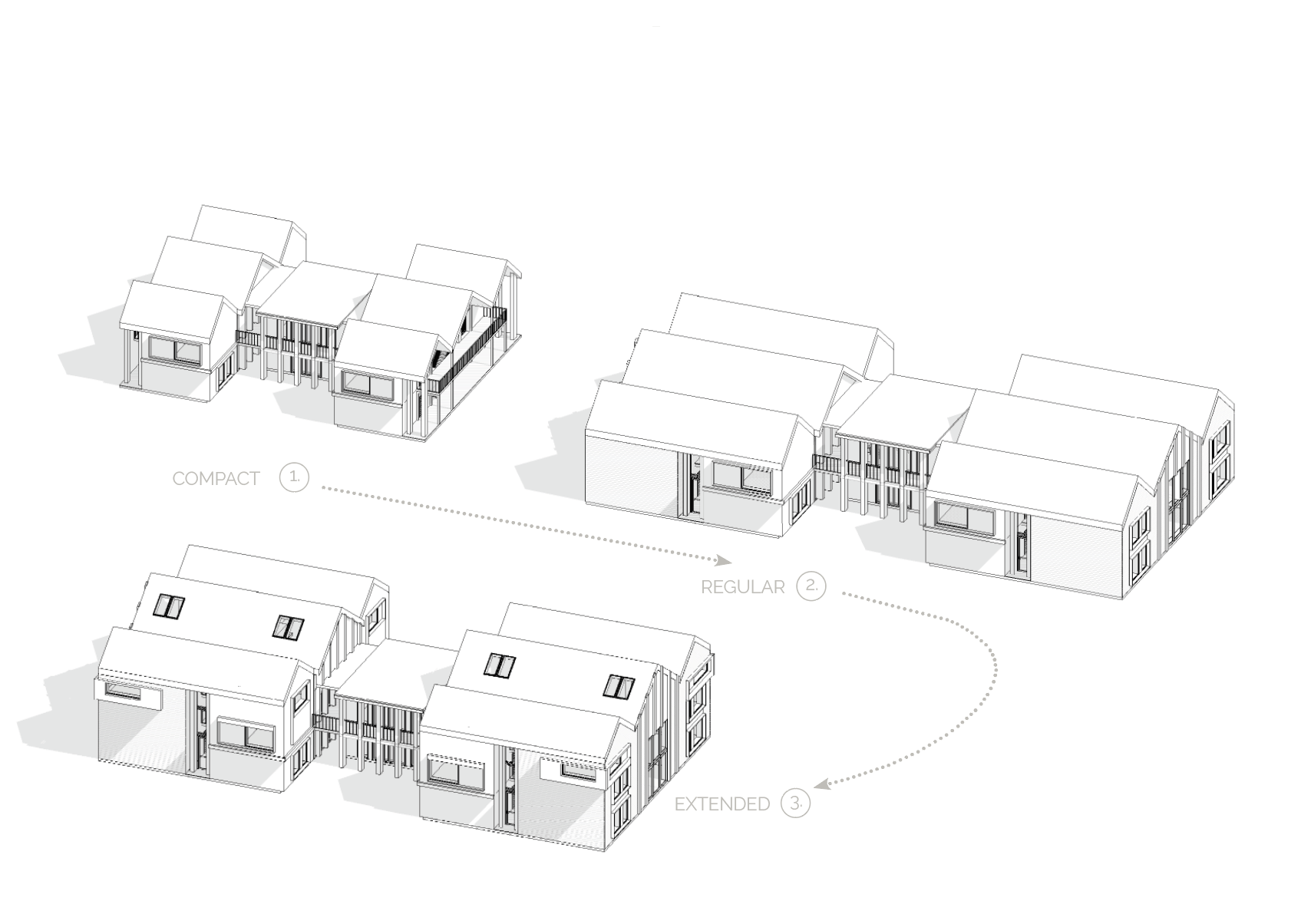



The COMPACT facility, aimed at being affordable, would only have the most needed functions, while the EXTENDED one, meant for bigger communities, could afford more additions.
The sizes also reflect in the architectural expression of the facility. The COMPACT one has a simplified version of the facade. It focuses on low cost construction and maintenance. It is therefore deprived of all redundant embellishments and other types of costly features. It is possible to later upgrade it to the REGULAR one, which allows for more leeway and the EXTENDED one, which assumes a budget that can cover some more ‘extras’. Also, the bigger the facility, the less rural setting it is aimed for.
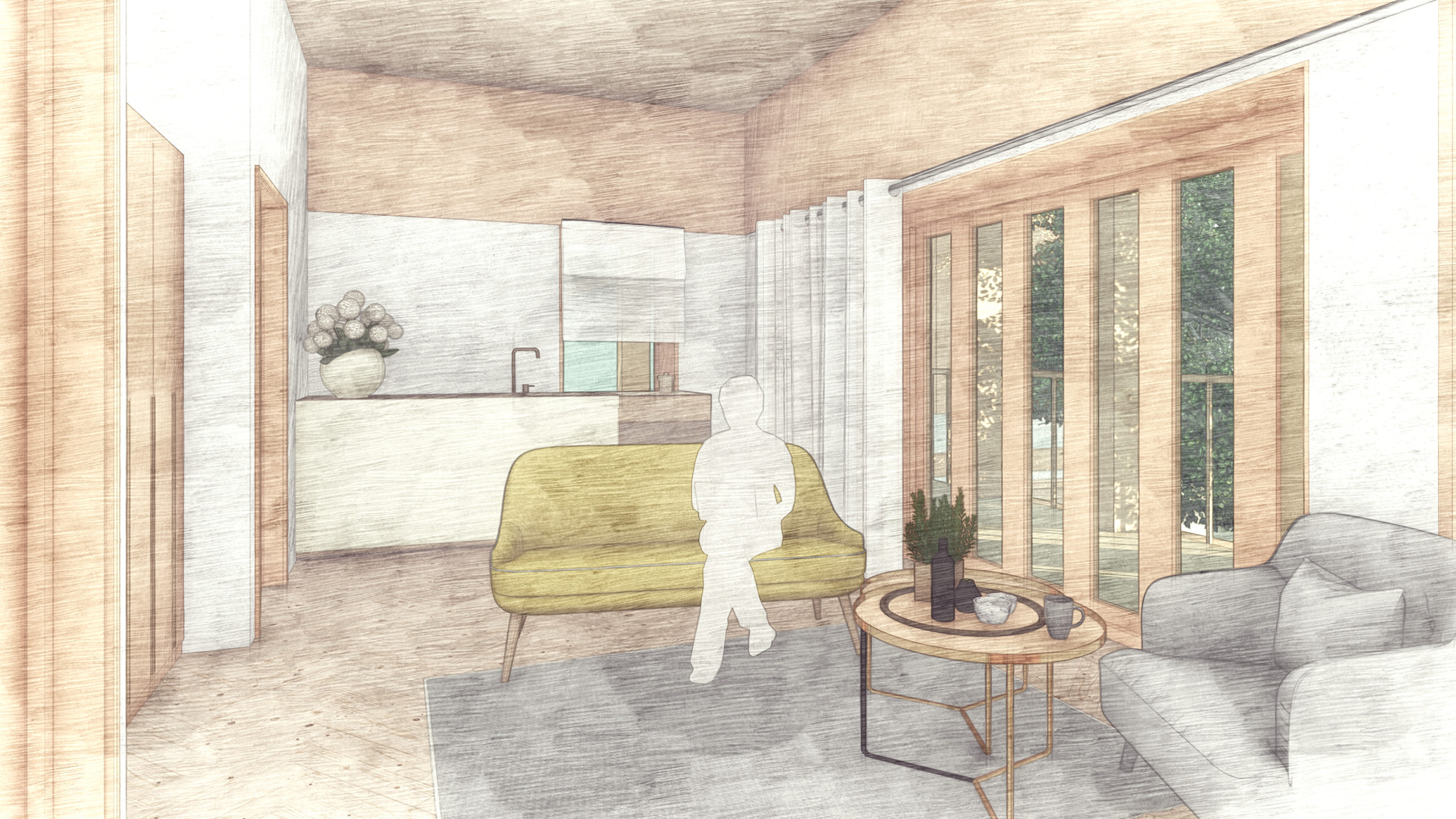
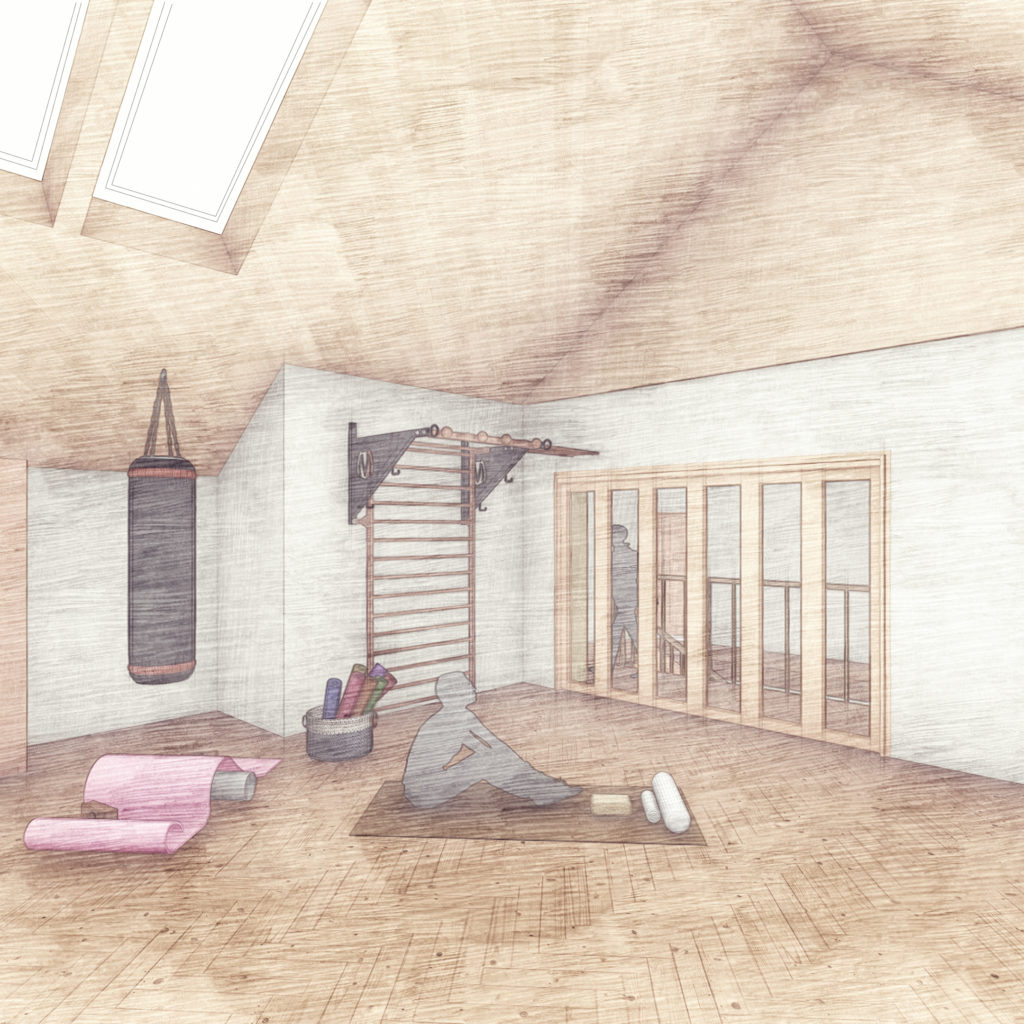
common spaces
The final proposal consists of range of spaces, which are an outcome of analysis of the patients needs, embedded in the expandable scheme.

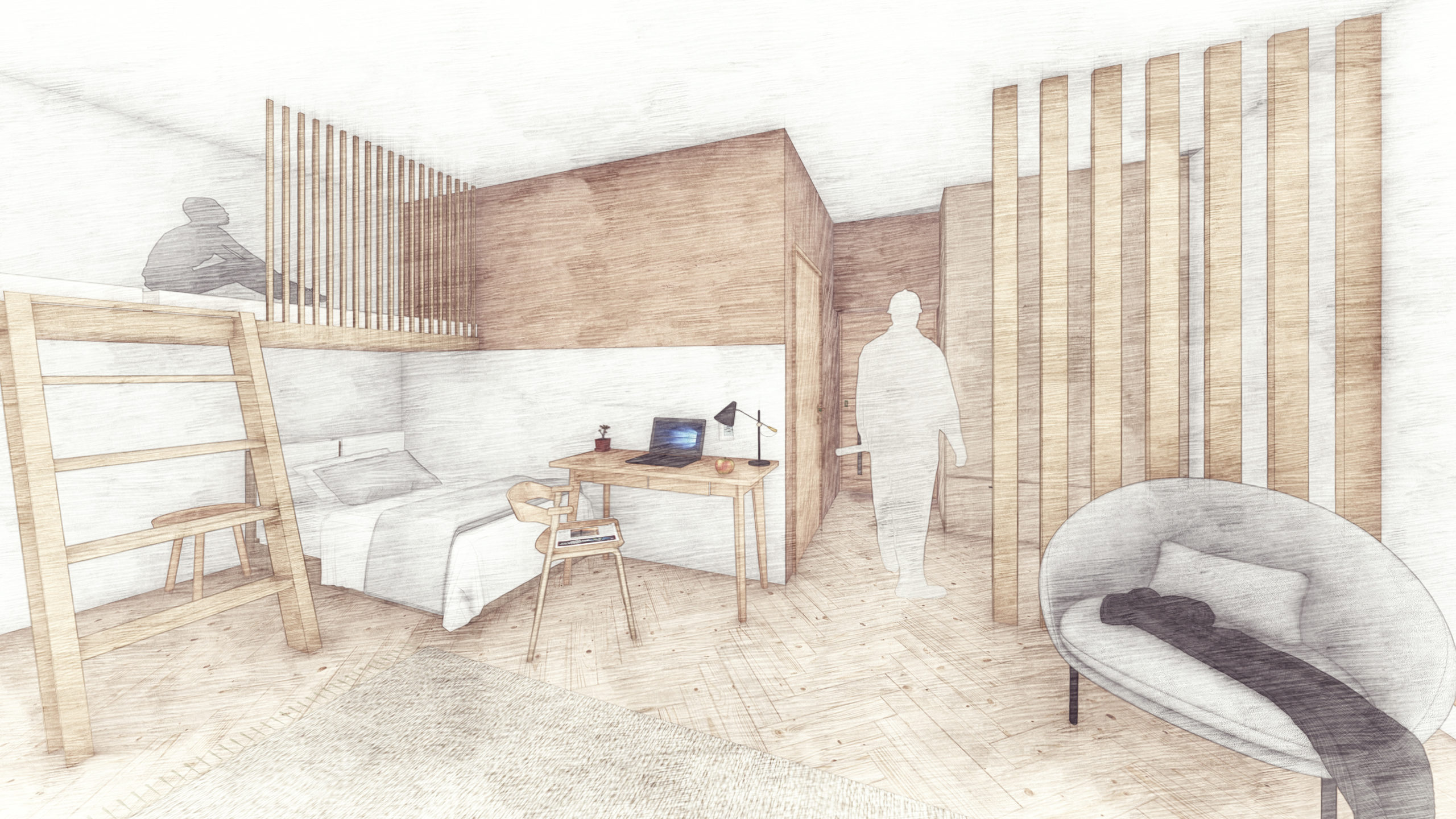
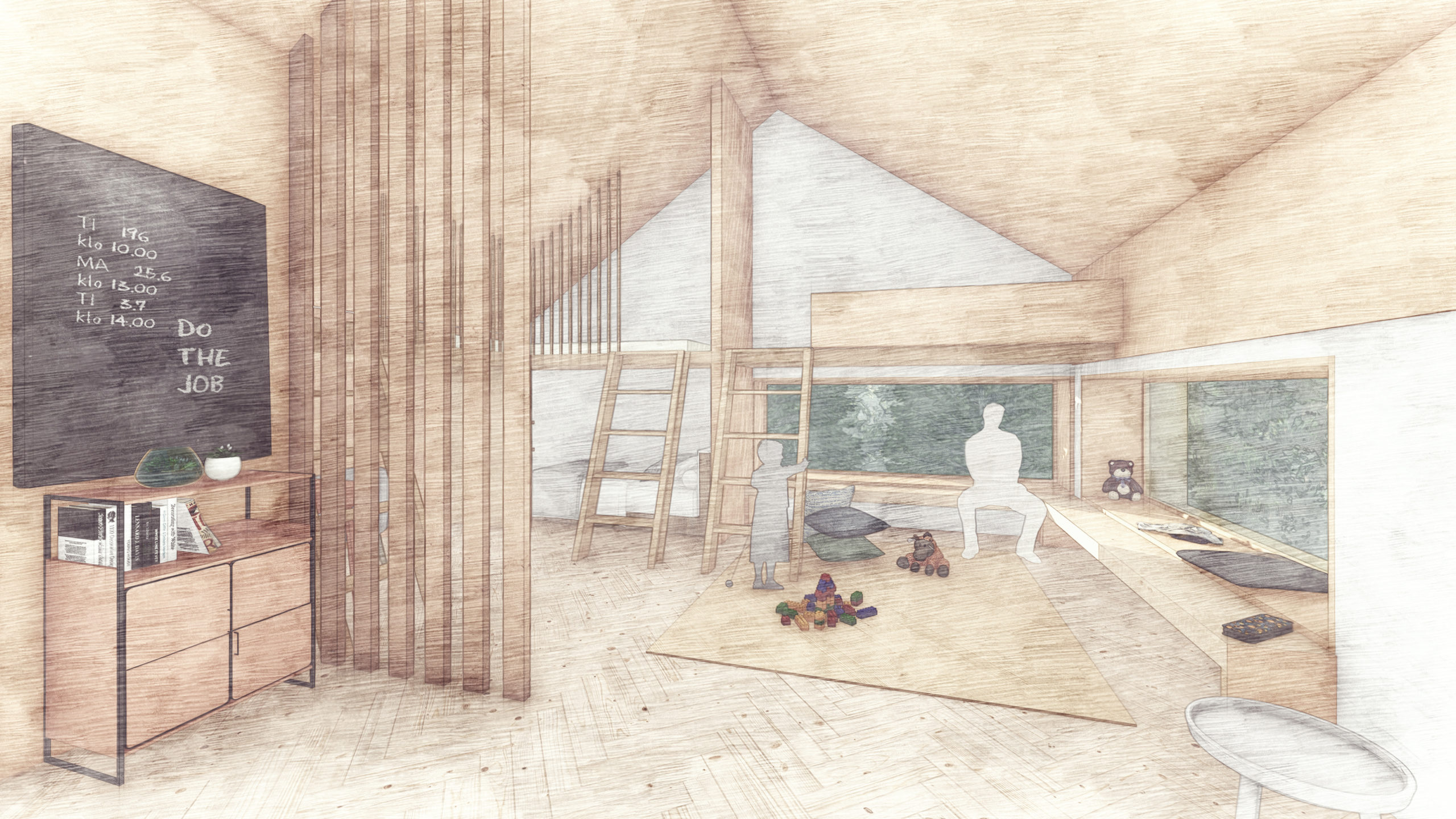
residents’ apartments

attachments
Please find the full version of the thesis below and learn more about the specific patient care solutions and the modular design performed in this project.
